SALZMANN'S NODULAR DEGENERATION
For an unknown reason, some eyes develop one or more creamy white nodular elevations called Salzmann’s nodules.
Call Us: 215-928-3180
 For an unknown reason, some eyes develop one or more creamy white nodular elevations called Salzmann’s nodules. These are often mild and located at the edge of the cornea, not causing any symptoms, and can simply be followed. However, if the nodules are larger or more central, they may cause irritation and/or decreased vision.
For an unknown reason, some eyes develop one or more creamy white nodular elevations called Salzmann’s nodules. These are often mild and located at the edge of the cornea, not causing any symptoms, and can simply be followed. However, if the nodules are larger or more central, they may cause irritation and/or decreased vision.
Lubrication, glasses, or contact lenses may be helpful. Occasionally surgical excision is warranted. Salzmann’s nodules can be removed with a blade or with an excimer laser (phototherapeutic keratectomy or PTK) with good success. The nodules sometimes recur after excision. The use of the anti-scarring agent mitomycin-C at the time of the procedure is believed to reduce the frequency and severity of recurrences.
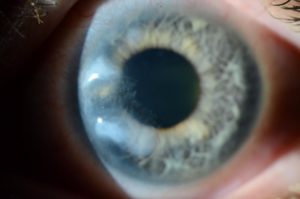
Single or multiple creamy white nodular elevations of the cornea. While they tend to start in the periphery, then can expand centrally.
Mild peripheral cases often asymptomatic. More advanced cases cause decreased or distorted vision with possible multiple or shadow images. Occasionally causes foreign body sensation and rarely pain.