DEFINITION
Ocular surface disease indicates damage to the surface layers of the eye, namely the cornea and conjunctiva. There are many causes ocular surface disease, but the 2 most common ones are “dry eye syndrome” and “blepharitis”.
SYMPTOMS
The most common symptoms of dry eye syndrome are a dry, gritty, sandy sensation in the eyes, but symptoms also include redness, mucous discharge, fluctuation of vision, contact lens intolerance, and ironically, excess tearing. Many of these symptoms can also be caused by other ocular conditions such as blepharitis (inflammation of the eyelids) and ocular allergies. Dry eye symptoms are often made worse by activities where patients tend not to blink frequently, such as reading, working on the computer, and watching television. Dry eye symptoms are also generally worse toward the end of the day.
Blepharitis symptoms are very similar to dry eye symptoms. Blepharitis tends to cause more redness and crusting of the eyelids and the symptoms are often worse in the morning and improve throughout the day.
CAUSES
Dry eye syndrome is primarily caused by poor quality or quantity of tears.
Blepharitis means inflammation of the eyelids. Blepharitis is often divided into anterior (involving the front aspect of the eyelids including the lashes) and posterior (involving the eyelid margin including the Meibomian glands). In reality, many eyes have both forms at the same time.
RISK FACTORS
Dry eye syndrome: advancing age, female, dry environment, smoking exposure, connective tissue disorder (e.g. Sjogren syndrome, rheumatoid arthritis), conjunctival scarring (e.g. from prior injury), certain medications (e.g. anti-histamines, beta-blockers), vitamin A deficiency, prior eye surgery, especially corneal refractive surgery.
Blepharitis: advancing age, rosacea, prior isotretinoin (e.g. Accutane) use
COMPLICATIONS
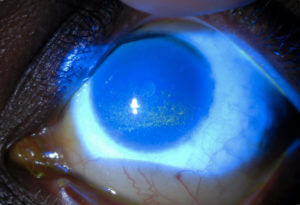
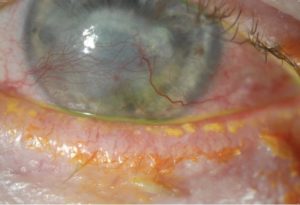
Corneal “dry spots”, corneal abrasions, corneal infections, corneal scarring, corneal thinning, corneal perforation.
TESTS AND DIAGNOSIS
The diagnosis can usually be made during a slit lamp examination with special dyes such as fluorescein and lissamine green. Ancillary testing includes measurement of tear production (Schirmer’s test), and possibly measurement of tear saltiness (osmolarity) and tear inflammation (e.g. MMP-9). If Sjogren syndrome is suspected, a referral to a rheumatologist should be considered.
TREATMENT
There is a stepwise approach treatment of dry eyes generally beginning with artificial teardrops, gels and ointments, cyclosporine drops (e.g. Restasis or Cequa), lifitegrast drops (e.g. Xiidra), and punctal plugs. Changing the local environment such as using humidifiers and staying away from drafts can also be very helpful. Other treatments include cautery of the tear drainage ducts (when plugs aren’t staying in), Lacriserts, acetylcysteine (Mucomyst) for mucous filaments, and permanent partial closure of the eyelids (small lateral tarsorrhaphy). Dry eye syndrome is often a chronic condition, but can usually be controlled with treatment.
Treatment depends partly on whether it is more anterior or posterior but generally includes a combination of warm compresses, eyelid scrubs, artificial tears, antibiotic drops or ointment, cyclosporine or lifitegrast and occasionally topical steroids or oral antibiotics. Blepharitis, like dry eye syndrome, is often a chronic condition, but can usually be controlled with treatment. For eyelid inflammation not responding to medical therapy, an in-office Lipiflow procedure can often improve dryness symptoms by clearing out the Meibomian glands.
PREVENTION
Routine eye examinations are recommended to monitor the condition.
 haritis
haritis